In a bustling industrial park on the outskirts of Accra, Ghana, technicians at Atlantic Lifesciences are calibrating bioreactors for a new round of vaccine trials—part of a quiet revolution unfolding across Africa. Once reliant on imports for nearly all its vaccines, the continent is now on the verge of producing its own, with 11 African-made vaccines expected to reach the market within five years. This milestone, revealed in a 2026 analysis by the Clinton Health Access Initiative (CHAI) in partnership with NRL Enterprise Solutions, marks a turning point in public health sovereignty. Yet, as facilities rise and technology transfers advance, a complex web of challenges threatens to slow momentum just as products near approval.
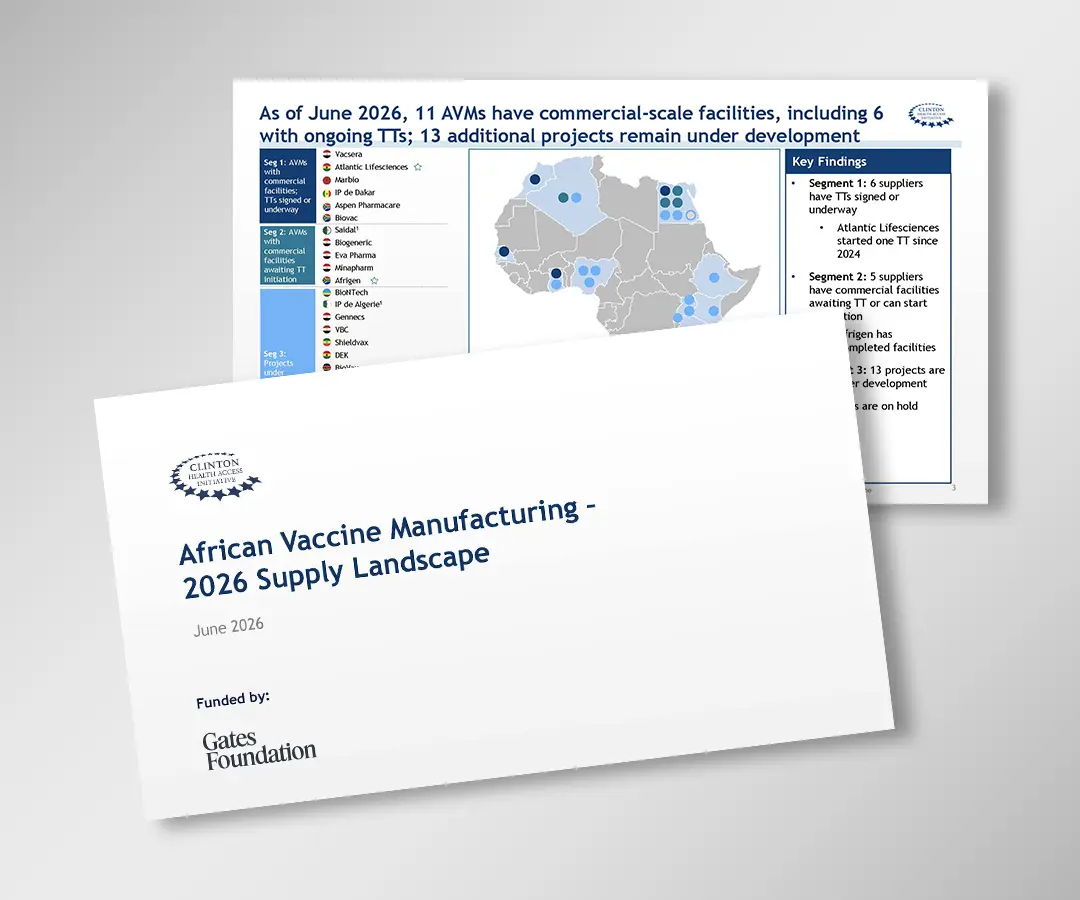
The vision is bold: by 2040, Africa aims to manufacture 60% of its vaccines domestically through the Partnerships for African Vaccine Manufacturing (PAVM). Since its launch, six manufacturers—including Atlantic Lifesciences, Afrigen Biologics in South Africa, and Uvax in Rwanda—have built facilities and initiated active technology transfer agreements. Some vaccines have already been licensed in their home countries, a sign of growing regulatory confidence. But reaching patients across the continent is proving far more difficult than anticipated.
Only one African manufacturer has submitted a filing to its national regulator for a product intended for broader continental use. Why? Because World Health Organization (WHO) prequalification—a critical benchmark—is just the first step. After that comes a fragmented patchwork of national registrations, UNICEF procurement negotiations, and ongoing compliance checks, each with unpredictable timelines. There is no standardized pathway, and no one knows how long it will take to navigate.
The CHAI report identifies five interlocking barriers: regulatory delays, uncertain demand, slow funding disbursement, stalled technology transfers, and workforce shortages. Worse, these issues amplify each other. A delay in financing can stall clinical trials, which pushes back regulatory submissions, which in turn dampens buyer confidence. Without clear procurement timelines from major buyers like Gavi or the African Union, manufacturers struggle to justify investment in scale-up.
The way forward demands coordination. Regulators must establish predictable approval pathways post-WHO prequalification. Donors and governments need to send stronger demand signals and align procurement with production timelines. And committed funds—like those from the Gates Foundation, which supported this research—must reach manufacturers faster, along with technical support for clinical development and workforce training.
This isn’t just about vaccines. It’s about building resilient health systems rooted in African innovation. As Dr. John Nkengasong, former Africa CDC director, once said, ‘You can’t secure health security from outside.’ The tools are being built. Now, the systems must catch up.